



Manfred Eggersdorfer, Ph.D. is a professor of healthy aging and holds the chair for healthy aging at the University Medical Center Groningen (UMCG) in the Netherlands and is the senior vice president responsible for nutrition science and advocacy of DSM Nutritional Products, in Kaiseraugst, Switzerland. He studied chemistry at the Technical University Munich and earned his Ph.D. in organic chemistry in the field of synthesis and characterization of unusual amino acids. He completed his post-doc at the Stanford-University, California, working with Carl Djerassi on the isolation and characterization of sterols from marine origin as potential contraceptives. He joined Roche, Basel, Switzerland in 1999 as head of research and development of vitamins and continued in this after Roche was acquired by DSM in 2003.
Dr. Eggersdorfer’s scientific work focuses on the role of essential nutrients for health, vitality and well-being, especially on the impact of inadequate intake and status of micro-nutrients on long term health and healthy aging. He is active as an advisory board member at the Johns Hopkins Bloomberg School of Public Health, member of the Nutrition Council of Tufts University Friedman School of Nutrition Science & Policy, Board member of the Gesellschaft für Angewandte Vitaminforschung e.V. and affiliate of various other organizations. He is the author of numerous publications in the fields of vitamins, innovation in nutritional ingredients and a scientific reviewer for a variety of journals.
Passwater:Can vitamin C kill cancer cells in cancer patients?
Eggersdorfer:As a nutrition expert, with a thorough understanding of the mechanisms of vitamin C, I am very well versed with the benefits of this micronutrient when consumed via dietary sources or as part of a supplement. For instance, there is significant research to indicate it can improve immune function and support general health and wellbeing (1). There is, however, also a growing body of evidence to suggest that vitamin C (ascorbic acid, or ascorbate), in pharmacologic concentrations, may be an effective tool in some cancer therapy treatments. Research groups are currently evaluating the potential and there is a lot of work still to be done. However, there are indications that this treatment is well-tolerated when used alongside radiation and chemotherapy methods, with some reports even suggesting it can enhance treatment outcomes (2). I very much look forward to seeing its future therapeutic potential become apparent.
Passwater:Now, a little background. There are reports in the scientific and medical literature of physicians using IV vitamin C dating back to 1940. Most of the early reports of clinical treatment of cancer patients with intravenous (IV) vitamin C that I have seen are by orthomolecular physicians such as Dr. Hugh Riordan and his colleagues at the Riordan Clinic in Wichita, KS. Few people have seen these very positive reports, but, on the other hand, many people have heard of the Linus Pauling and Cameron studies with vitamin C and cancer. And, perhaps even more have been told incorrectly that their studies were not confirmed. Basically, what did the Drs. Pauling and Cameron studies consist of?
Eggersdorfer:The observational studies initiated in 1974 by Drs. Cameron and Campbell, and later expanded with Dr. Pauling in 1976, investigated the suggestion that vitamin C could play a role in treating advanced cancer patients (3). This trial saw 100 terminal cancer patients receive “pharmacologic” doses of vitamin C as their only definitive form of treatment, and compared their progress to 1,000 identically-treated patients who did not receive any vitamin C. They reported that vitamin C supplied intravenously, and later orally, at doses of 10 g/day could prolong the survival of advanced cancer patients by up to 4.2 times, or 210 days (4). This study was instrumental in providing a foundation for later exploration of the clinical benefits of pharmacologic vitamin C and remains a milestone in the research timeline.
Passwater:A short clinical trial was conducted at the Mayo Clinic, but unfortunately, it wasn’t a true replication of the Pauling/Cameron trial. What were the important differences?
Eggersdorfer:Indeed, when Drs. Cameron and Pauling’s’ findings were later revisited by researchers at the Mayo Clinic, the results were not quite as expected. Their conclusions were deemed fallible due to multiple procedural uncertainties. The Mayo Clinic trial, using oral doses of vitamin C (rather than IVC), found no determinable benefit on cancer patients with respect to improvement of symptoms, performance status or survival (5, 6). However, the crucial difference between these two standpoints was that, in these later double-blind trials, only oral intake of vitamin C was used, whereas both oral and intravenous (IV) vitamin C doses had been provided in Drs. Cameron and Pauling’s’ studies (7). As a result, it is not possible to directly compare these findings. Today the scientific literature supports that only IV application may have an anticancer effect.
Passwater:So, the scientific literature supports that only high-doses of vitamin C given intravenously can raise the cellular levels sufficiently to kill cancer cells while leaving non-cancerous cells healthy.
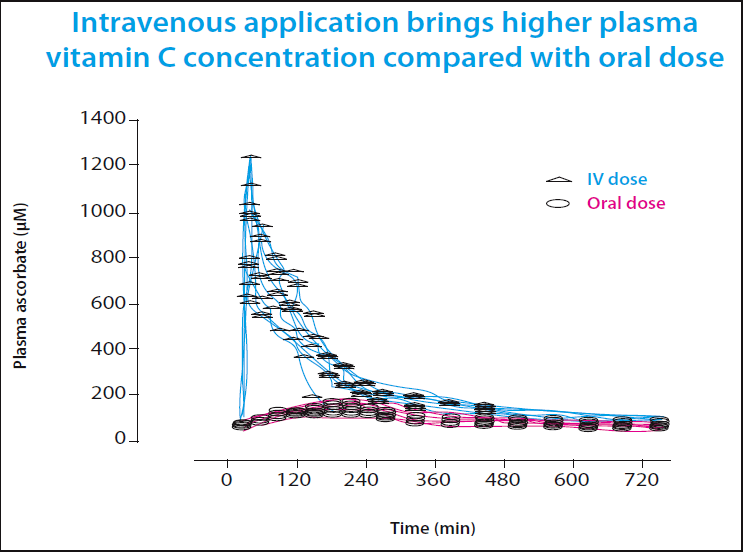
Eggersdorfer:Indeed, the method of delivery is an important factor, as identified by the controversy surrounding these early vitamin C trials. Emerging evidence increasingly supports the suggestion that IV infusion of vitamin C is more effective than oral dosage in regard to killing cancer cells, with reports indicating that the plasma vitamin C concentrations required for cancer therapy treatment are only achievable via IV dosage. In fact, numerous pharmacokinetic studies on healthy men and women indicate that IV injections can bypass the biological tight control that limits ascorbate concentration in oral doses to below 0.2 mM, or 200 µM, facilitating plasma ascorbate concentrations up to 70 times greater than is possible with oral dosing only (8, 9, 10).
Passwater:There are many beneficial actions of vitamin C. Why is such a high level of vitamin C required to kill cancer cells? What is the main biochemical mechanism involved?
Eggersdorfer:The bypassing of tight control of vitamin C absorption is a crucial mechanism in enabling vitamin C infused via IV to target the cancerous cells. Vitamin C, when it enters the body, breaks down easily in the cell’s extracellular fluid, creating (relatively weak) ascorbate free radicals and hydrogen peroxide (H2O2), a reactive oxygen that can damage tissue and DNA. The important factor that enables vitamin C to be utilized in cancer therapy treatments is that healthy cells are rich in the enzyme catalase, which rapidly disposes of hydrogen peroxide and protects the cell. Cancerous cells, on the other hand, are severely deficient in catalase and are unable to defend against the hydrogen peroxide’s attack, meaning that they are damaged and killed. It is via this mechanism that pharmacologic vitamin C can selectively target tumorous cells during cancer treatment, if a high-enough concentration of vitamin C is achieved inside the tumors (11, 12).

Passwater:Have recent clinical studies shown benefit of IVC against cancer and more or less confirmed the older Drs. Pauling and Cameron findings?
Eggersdorfer:While this research is still ongoing, the existing evidence does suggest that IV vitamin C can have a significant impact on patients, without any adverse side effects on health or wellbeing. Studies by Welsh (2014) and Yun et al. (2015) are just some examples of trials that have indicated an improvement in quality of life and physical, mental and emotional functions, as well as symptoms of fatigue, nausea, vomiting and pain in cancer patients, although it is widely recognized that therapy is needed over a longer period of time to maximize efficacy (13, 14).
Passwater:Can you give us an example of a study showing that vitamin C kills cancer cells?
Eggersdorfer:With this research continuously gaining traction, evidence continues to emerge that highlights the potential of vitamin C in killing cancerous cells. A particularly notable study is that by Yun et al. (2015), which examined colorectal cancers carrying either KRAS or BRAF gene mutations that contribute to tumor growth. The findings indicated that colorectal cancer cells harboring these mutations are selectively killed when exposed to high levels of vitamin C, as a result of specific targeting and inhibition of glyceraldehyde 3-phosphate dehydrogenase (GAPDH). This mechanism facilitates cellular energy depletion in mutated cancerous KRAS and BRAF cells, ultimately leading to cell death (15).

Passwater:Slowly, but surely, additional research with IV vitamin C and cancer has been conducted at one of the USA’s leading health institutes, the National Institutes of Health in Bethesda, MD. Please tell us a little about this research.
Eggersdorfer:Indeed, there is a lot of ongoing research into the potential of IV vitamin C in cancer treatment, not just in Maryland but in universities and medical centers across the globe. The University of Otago in Christchurch, New Zealand, the Maastricht University Medical Center in The Netherlands and the University of Miami Miller School of Medicine in Miami, FL, are just a few examples of the organizations at the forefront of this pioneering research. At DSM, we have a long history of supporting clinical trials with our ingredients, because we know that an important factor in maximizing the success of these studies is ensuring the quality of the active pharmaceutical ingredients (APIs). With providers of high quality, pharmacologic IV vitamin C in short supply, we are committed to continue our collaboration to support the future of this research.
Passwater:There is no doubt, however, that IV vitamin C is critical for killing cancer cells, whereas oral vitamin C may only bring about quality of life improvements. The 1996 Levin study mentioned earlier involved only seven healthy, young, male volunteers, aged 20 to 26, who were in a hospital for a period between four to six months. The 2001 study similarly involved 15 healthy young females. Care must be taken in expanding these data to represent an entire population. Readers may want to keep in mind the findings of Dr. Robert Cathcart who reports that vitamin C absorption varies with body needs and disease states. (Please refer to last month’s interview with Dr. Andrew Saul regarding the findings of Dr. Cathcart.)

Vitamin C absorption studies are complex and not easily carried out. The following comments are not intended to be critical, as Drs. Steve Hickey, Hilary Roberts and myself greatly admire the excellent research by Dr. Mark Levine with vitamin C and cancer. As constructive comment on page 82 of their 2004 book, “Ascorbate: The Science of Vitamin C,” Drs. Hickey and Roberts point out that the plasma levels reported by Dr. Levine are not saturation levels.
In chemistry, the common usage of “saturation” means that the blood holds as much vitamin C as it is possible for it to hold. Drs. Hickey and Roberts comment in their book, that “This is far from true. The base plasma levels tended to stabilize at a dose of around one gram a day, at which point it was claimed that the plasma was ‘saturated.’” This might be taken to imply that higher doses of vitamin C did not raise the blood levels; however, Dr. Levine’s own data show that they do, as can be seen from Figure 5.
As Drs. Hickey and Roberts point out, to obtain steady-state blood levels of vitamin C, the dose intervals must be similar to the length of time it takes to excrete the vitamin. The half-life (the time for one-half of the blood content to be excreted) of vitamin C is very short. This is the reason that it is usually recommended to divide one’s daily intake of vitamin C into several smaller doses rather than a single larger dose of the same amount. The absorption efficiency is increased resulting in a greater percentage of vitamin C being absorbed and also, the blood levels are more level. However, as Dr. Levine relates, it is difficult to get volunteers to take frequent multiple doses at short intervals and to have blood samples taken at each one.

Drs. Hickey and Roberts also point out that Dr. Levine’s absorption studies that are so widely quoted as being “definitive” may be flawed because of the vitamin C blood half-life. The so-called “steady-state” plasma and tissue concentrations at seven vitamin C dose levels, ranging from 30 to 2,500 milligrams per day also excluded the higher doses recommended by Drs. Pauling and Cameron. And others. The plasma measurements were made each day before subjects received their vitamin C.
According to Drs. Hickey and Roberts, this meant that the measurements were taken when the vitamin C had been excreted. These readings would merely measure the background level of vitamin C in the blood and not the peak of even average values as claimed. I would hope that since these studies are so fundamental and so important, that a larger study with a better protocol be sponsored to obtain this vital information.
Also, the effect of liposomal vitamin C on blood levels of vitamin C should be further explored. Liposomal vitamin C is believed to bypass the tight regulation of vitamin C absorption because it “protects” vitamin C molecules by “encapsulating” them with phospholipids.
In any event, there is no question that direct IVC raises blood levels of vitamin C sufficiently to kill at least some types of cancer cells and without harming normal cells. Our next two columns will discuss the exciting research that has systematically been carried out at the Riordan Clinic in Wichita, KS over the decades. We will first chat with Dr. Ron Hunninghake and then Dr. Nina Mikirova.
Dr. Eggersdorfer, once again we thank you for discussing the basic biochemistry of intravenous vitamin C against cancer. We look forward to our next discussion.WF
References1. Henson et al. “Vitamin c: a new look”Ann. Intern. Med., vol. 114, no. 10, 1991, p. 909-910. 2. H. Fritz et al. , “Intravenous Vitamin C and Cancer: A systematic review,”Integrative Cancer Therapies, vol. 13, p. 280-300 (2014). 3. E. Cameron and A. Campbell, “The orthomolecular treatment of cancer: clinical trial of high-dose ascorbic acid supplements in advanced human cancer,”Chem.-Biol. Interactions, vol.9, no. 1, p.285-315 (1974). 4. E. Cameron and L. Pauling, “Supplemental ascorbate in the supportive treatment of cancer: prolongation of survival times in terminal human cancer,”Proc. Natl. Acad. Sci. USA, vol. 73, no. 10, p. 3685-3689 (1976). 5. E. T. Creagan et al. , “Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer,”New England Journal of Medicine, vol. 301, no. 13, 1, p.687-690 (1979). 6. C.G. Moertel et al. , “High-dose vitamin C versus placebo in the treatment of patients with advanced cancer who have had no prior chemotherapy,”New England Journal of Medicine, vol. 312, no. 3, p.137-141 (1985). 7. M. Levine et al. , “Losing and finding a way at C: New promise for pharmacologic ascorbate in cancer treatment,”Free Radic Biol Med., vol. 47, no. 1, p.27-29 (2009). 8. M. Levine et al. , “Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance,”Proc. Natl. Acad. Sci, vol. 93, no. 1, p.3704-3709 (1996). 9. M. Levine et al. , “A new recommended dietary allowance of vitamin C for healthy young women,”Proc. Natl. Acad. Sci, vol. 98, no. 17, p. 9842-9846. (2001). 10. S.J. Padayatty et al. , “Vitamin C pharmacokinetics: implications for oral and intravenous use,”Ann. Intern. Med., vol. 140, no. 7, p.533-537 (2004). 11. N. H. Riordan et al. , “Intravenous ascorbate as a tumour cytotoxic chemotherapeutic agent,” Medical Hypotheses, vol. 44 no. 1, p. 207-213 (1995). 12. Doskey et al. , “Tumor cells have decreased ability to metabolize H2O2: implications for pharmacologic ascorbate in cancer therapy,”Redox Biology, vol. 10, no. 1, p. 274-284 (2016). 13. J.L. Welsh et al. , “Pharmacologic ascorbate with gemcitabine for the control of metastatic and node-positive pancreatic cancer,”Cancer chemotherapy pharmacology, vol. 71, no. 13, p. 765-775 (2013). 14. J. Yun et al. “Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells by targeting GAPDH,”Science, vol. 350, no. 6266, p. 1391-1396 (2015). 15. Ibid. 16. Hickey, S. and Roberts, H. “Ascorbate: The Science of Vitamin C,” p. 82, Lulu.com Publ. ISBN: 97814116072486 (2007).

Dr. Richard Passwater is the author of more than 45 books and 500 articles on nutrition. Dr. Passwater has been WholeFoods Magazine’s science editor and author of this column since 1984.
NOTE: The statements presented in this article should not be considered medical advice or a way to diagnose or treat any disease or illness. Dietary supplements do not treat, cure or prevent any disease. Always seek the advice of a medical professional before adding a dietary supplement to (or removing one from) your daily regimen. The opinions expressed in bylined articles are not necessarily those of the publisher.
Published in WholeFoods Magazine March 2018








