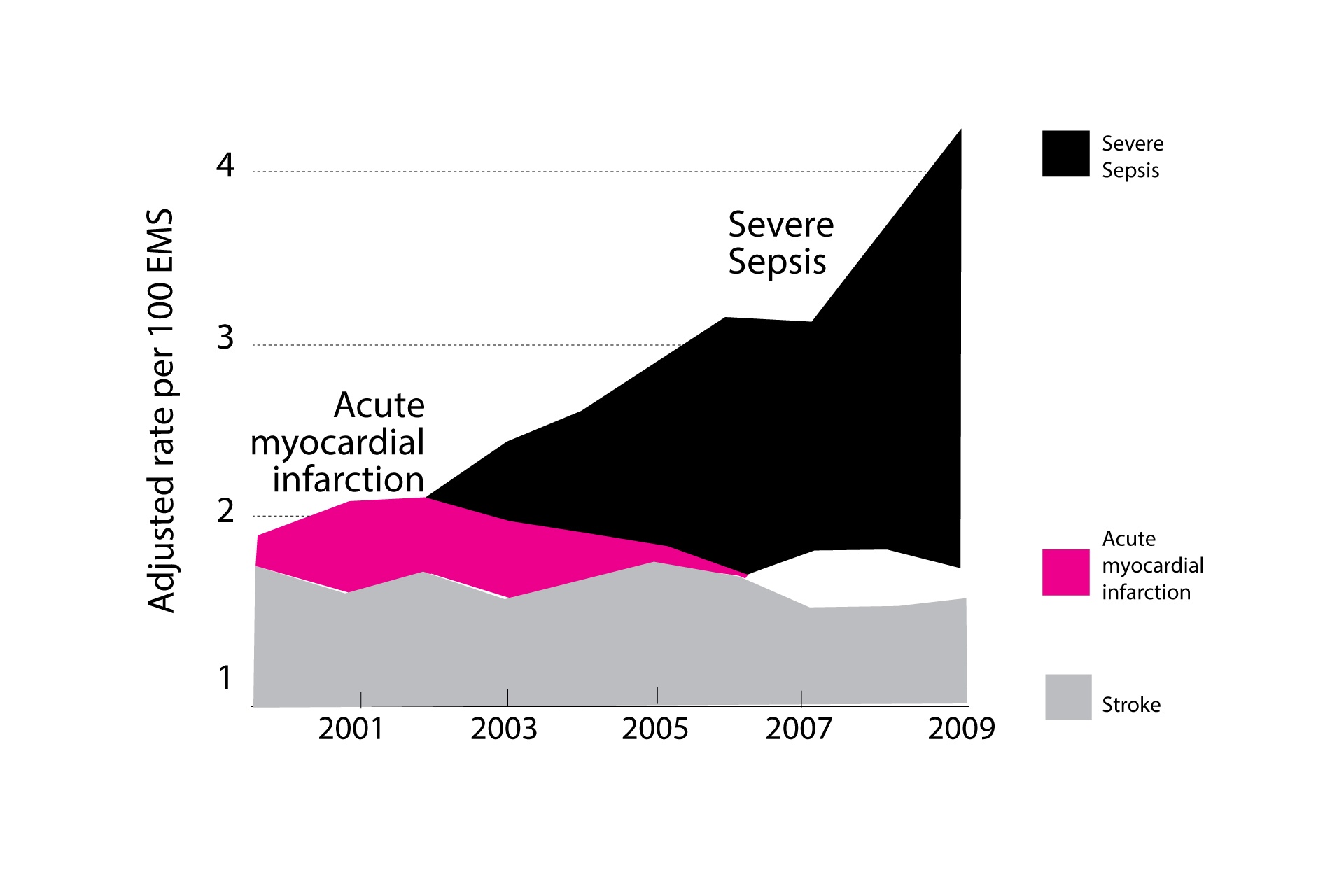
Severe sepsis strikes more than a million Americans every year, and 15 to 30 percent of those people die. (2) The Centers for Disease Control put the figure at 1.5 million Americans getting sepsis and about 250,000 dying from it. (3) They also report that one in three patients who die in a hospital have sepsis. (3) How many have you known? The World Federation of Pediatric Intensive and Critical Care Societies (WFPICCS) estimates that 30 million die from sepsis worldwide. (4) Many of those who don’t die have such damaged organs that they have their lives shortened. It is estimated that 40 percent of sepsis patients are readmitted to the hospital within three months. (5) The number of sepsis cases per year has been on the rise in the United States. (6)
According to the National Institutes of Health, sepsis is a major challenge in hospitals, where it’s one of the leading causes of death. It is also a main reason why people are readmitted to the hospital. Patients are too-often admitted to a hospital with a routine infection only to end up dying of sepsis.
It has been known for decades that vitamin C can help cure sepsis. Until relatively recently, this fact has been largely ignored by orthodox physicians.
Sepsis has been a concern of mine, as well as that of my younger son, Michael. Mike has been involved in studying blood professionally for more than 26 years and has closely followed the research with vitamin C and sepsis. I have taken the opportunity to call upon Mike to chat with us about the history of vitamin C and sepsis and some of the recent developments.
Michael E. Passwater is certified by the American Society for Clinical Pathology as a Medical Technologist, a Specialist in Blood Banking, and a Diplomate in Laboratory Management. He is a Certified Six Sigma Green Belt by the American Society for Quality, and has a patient blood management certificate from the Society for the Advancement of Blood Management. He has worked in clinical laboratories for 26 years.
Richard Passwater:Why did you choose a career in Clinical Laboratory Science?
Mike Passwater:I grew up in a home that emphasized learning, caring, working, quality over quantity, and service. My parents were both busy professionals who were also volunteer Emergency Medical Technicians (EMTs) for our community fire and rescue squad. My brother was also a volunteer firefighter/first responder and worked as a life guard during his school years. In early adolescence, I encountered the HIV/AIDS pandemic in the news. T cells, B cells, and the concept of the immune system as a mobile organ that interacted with all the other organs fascinated me – and still does. My high school chemistry teacher took us on a field trip to the local hospital (30 minutes away in another county), and I learned of a connection between classes I enjoyed and employment opportunities in hospitals helping people.
In my sophomore year at the University of Delaware, I switched from a research-oriented Chemistry program to the applied science of Medical Technology. The following semester I took my first immunology course studying Ivan M. Roitt’s Essential Immunology text with a dynamic, encouraging professor. I was hooked. Upon graduation, the largest hospital in the area hired me to work in the blood bank (aka immunohematology) section of their clinical laboratory. Solving antibody – antigen puzzles, having an ancillary role supporting emergency medicine and critical care activities, and keeping up with the rapidly developing fields of immunology, transfusion medicine, and transplantation remains a fascinating journey.
R. Passwater:Many, if not most, are unaware of the killer called sepsis. Just what is sepsis?
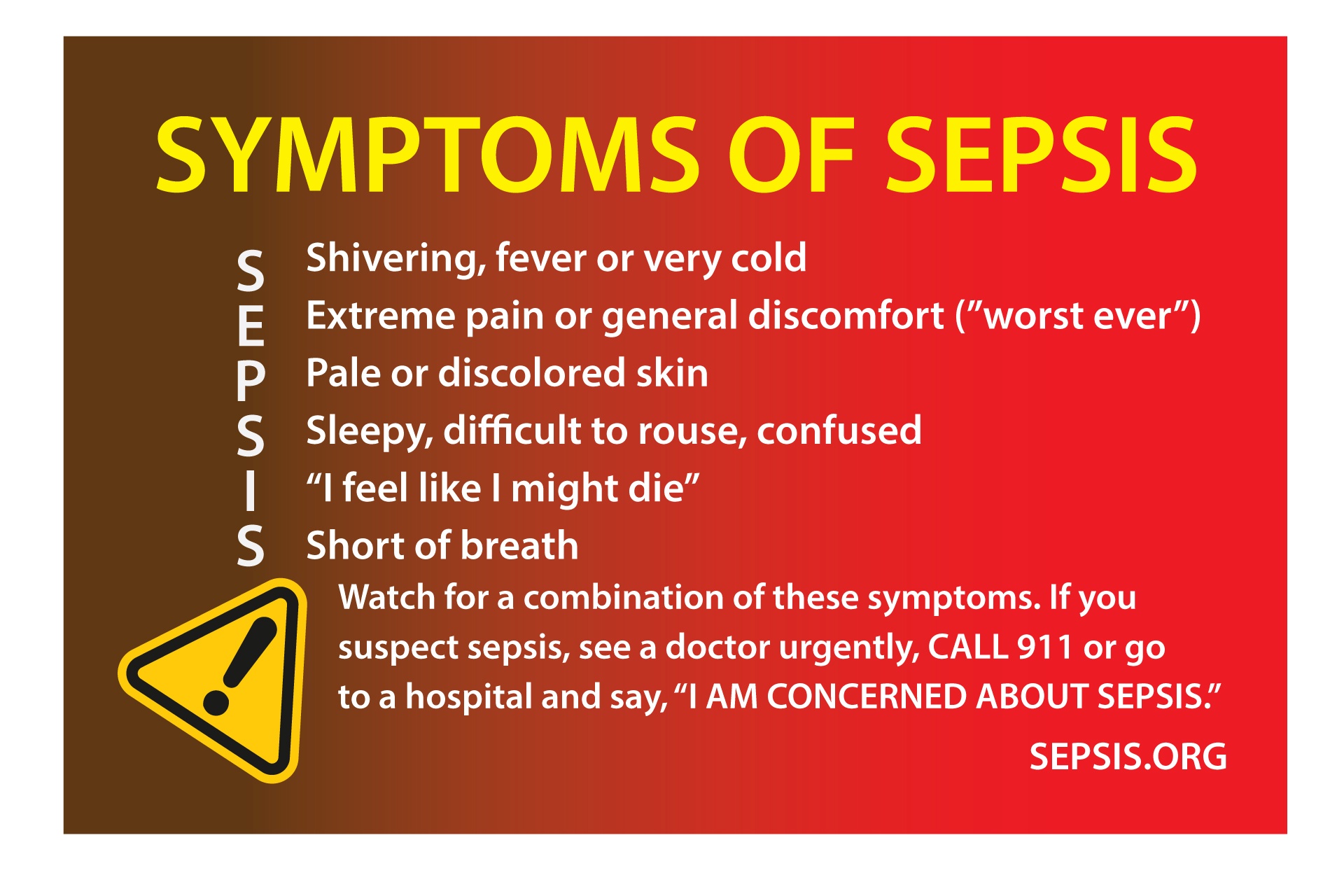
Mike Passwater:Sepsis is gaining needed attention. The Sepsis Alliance (www.sepsis.org) was founded in 2007 in memory of Dr. Carl Flately’s daughter Erin, who died of sepsis at the age of 23. It is active raising money and awareness in all 50 states. In 2013, “Rory’s Regulations” became law in the state of New York. Rory Staunton died of sepsis at the age of 12. The regulations require hospitals in New York to consider sepsis present until it can be ruled out, and to complete standardized sepsis checklists as part of patient assessments.
 The terms sepsis, septic shock, and systemic inflammatory syndrome (SIRS) are useful for this discussion. The Merck Manual defines sepsis and septic shock as follows:
“Sepsis is a clinical syndrome of life-threatening organ dysfunction caused by a dysregulated response to infection.”
The terms sepsis, septic shock, and systemic inflammatory syndrome (SIRS) are useful for this discussion. The Merck Manual defines sepsis and septic shock as follows:
“Sepsis is a clinical syndrome of life-threatening organ dysfunction caused by a dysregulated response to infection.”“Septic shock is a subset of sepsis with significantly increased mortality due to severe abnormalities of circulation and/or cellular metabolism. Septic shock involves persistent hypotension (defined as the need for vasopressors to maintain mean arterial pressure equal or greater than 65 mm Hg, and a serum lactate level greater than 18 mg/dL [2 mmol/L] despite adequate volume resuscitation.” (8)
 Sepsis is an infection that overwhelms the body. Widespread inflammation – caused by the infection and by the immune system’s attempts to destroy the infection – along with metabolic acidosis result. Various populations of white blood cells often become hyperactive and then may self-destruct. If untreated, sepsis may lead to shock, organ failure, and death. Sepsis is a medical emergency.
Sepsis is an infection that overwhelms the body. Widespread inflammation – caused by the infection and by the immune system’s attempts to destroy the infection – along with metabolic acidosis result. Various populations of white blood cells often become hyperactive and then may self-destruct. If untreated, sepsis may lead to shock, organ failure, and death. Sepsis is a medical emergency.For over a half century, surgeons have recognized that sometimes following major trauma or surgery, widespread inflammation and metabolic acidosis may occur even in the absence of infection. The term “sterile sepsis” was used to describe this syndrome. However, the newer term “Systemic Inflammatory Response Syndrome” is now more commonly used to describe both a sepsis-like picture not associated with infection, and early sepsis. Common to these scenarios as they worsen are hypotension (low blood pressure), relative adrenal insufficiency, and metabolic acidosis. Another commonality is low plasma levels of vitamin C (ascorbic acid). Borrelli et al published findings in 1996 showing that the lower the plasma ascorbic acid level in septic patients, the greater the risk of organ failure and death. (9)
What does any of this mean? Our bodies have approximately 60,000 miles of blood vessels – arteries, capillaries, and veins carrying our blood from our heart to our lungs, to our tissues, and back again. We have about five liters of blood being pushed around this circuit every minute. Our blood vessels are not inert tubes. They are lined with special cells called endothelial cells, and a thin protective coating called the glycocalyx covers the inside of these cellular tubes. (10)
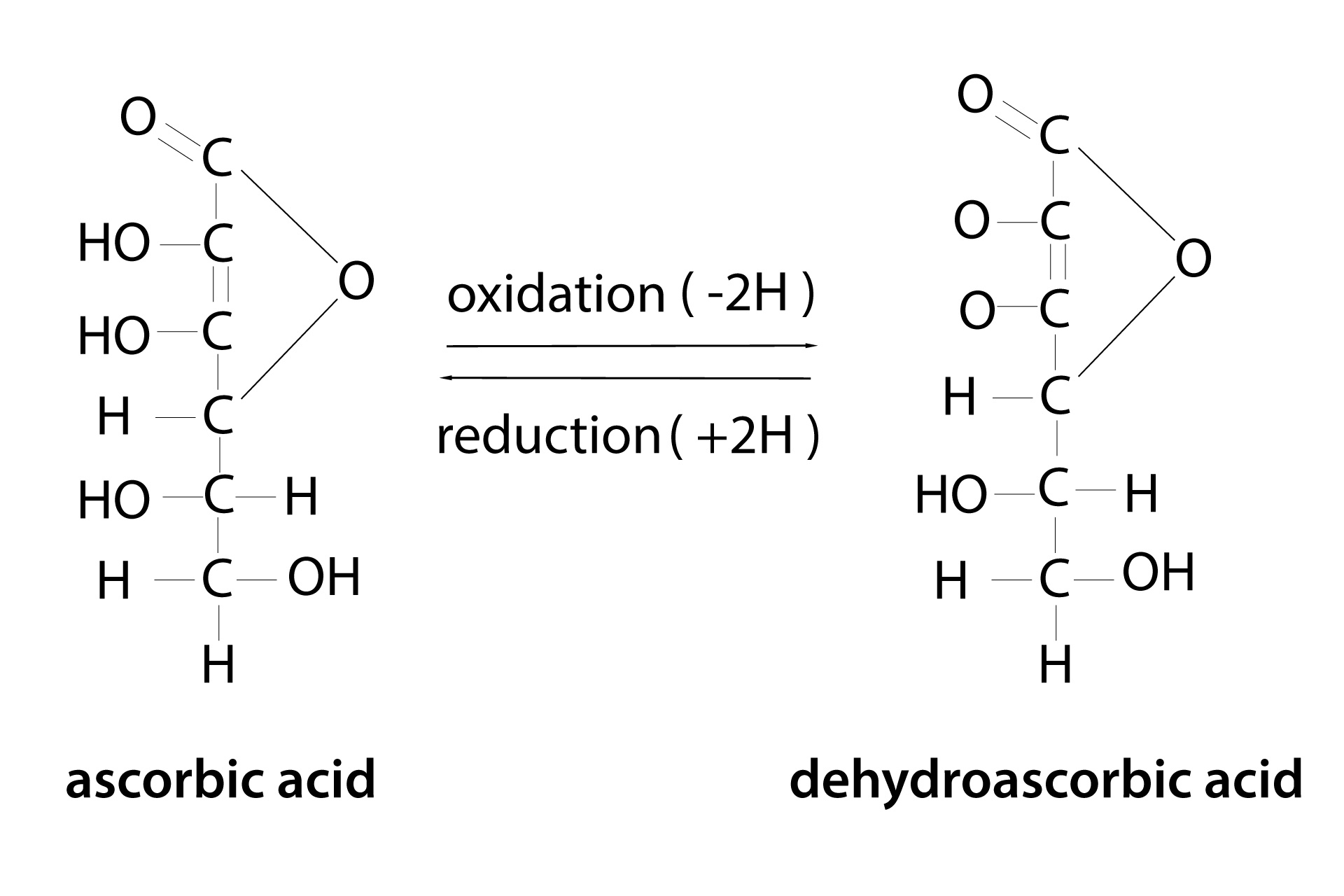
Healthy adults have roughly 20-30 trillion red blood cells circulating in our 5 liters of blood. As red blood cells mature and enter the blood circulation in humans (and other mammals incapable of making their own vitamin C), the number of GLUT1 transport receptors (a major receptor for uptake of glucose [blood sugar] and oxidized Vitamin C) increases by 1,000-fold and is co-expressed with the membrane protein stomatin. This configuration on the red blood cell membrane switches GLUT1 from a glucose transporter to a Dehydroascorbic Acid (DHAA) transporter. (11) DHAA is the oxidized form of ascorbic acid (AA) and is preferentially transported into the red blood cells where it is reduced (recycled) back to vitamin C (Ascorbic Acid) and released into the circulation. (Please see Figure 3.) Ascorbic Acid (AA) is preferentially transported into endothelial cells, white blood cells, platelets, and other cells via the SVCT2 transport receptors. Vitamin C as AA is important to maintain the integrity of the endothelium, and it also is important for powering white blood cells and other components of the immune system. In addition to being an antioxidant itself, vitamin C (AA) also has epigenetic (gene activity and expression) effects including activation of the nrf2 antioxidant pathway. Furthermore, vitamin C (AA) is necessary for the body to produce catecholamines including epinephrine (“adrenaline”) and norepinephrine, and it impacts the production of cortisol.
If you don’t want leaky blood vessels and collapsing blood pressure, you need adequate vitamin C. Without vitamin C, the white blood cells and adrenal proteins become depleted, blood vessels weaken, circulation weakens, and the situation eventually becomes life-threatening. Vitamin C (AA) has a brief half-life of several minutes in healthy plasma before it is oxidized to DHAA. The DHAA-AA recycling process optimizes the body’s ability to survive on the meager amount of ascorbic acid in the typical human diet. In the brain, a similar recycling process exists between astrocytes and tanycytes with GLUT1-DHAA receptors and neurons with SVCT2-AA receptors.
Infections and inflammation increase consumption of vitamin C, and disrupt the recycling processes the body uses to conserve this essential nutrient. Once AA is depleted, blood vessels begin to weaken and become leaky. Adding back in “pressors” (e.g. epinephrine) alone, or even with cortisol (hydrocortisone), is not enough. This is where the work of Dr. Richard E. Lee in the 1950s – 1960s comes into play. We can chat more about that later.
R. Passwater:Who is most at risk for sepsis?
Mike Passwater:People born with incomplete immune systems, or those that acquire immune system deficits through illnesses such as HIV or blood cancers (e.g. leukemia, lymphoma, myeloma), or due to chemotherapy greatly lowering the bone marrow production of white blood cells. Other serious illnesses such as cirrhosis and diabetes also increase the risk of sepsis. Children, the elderly, anyone with malnutrition, or anyone with a persistent serious infection is at increased risk of developing sepsis. It is important to note that some severe illnesses can cause a healthy, active person to progress to sepsis and septic shock in a short period of time.
R. Passwater:What attracted your interest to vitamin C?
Mike Passwater:Vitamin C isn’t pixie dust or magic, but it is a critical factor in a wide range of biochemical processes throughout the human body. And, like all essential nutrients, it must be delivered into the body for the body to stay alive. It is water-soluble and has a short half-life. For these reasons, it can be the rate-limiting factor in many biological processes.
Drs. James May and Fiona Harrison detailed seven known molecular functions of vitamin C and associated relevance in 2013: (12)
1. Primary antioxidant• scavenges damaging radicals
2. Pro-oxidant• redox regulation • DNA, or protein damage
3. Recycling• numerous, including chain breaking of lipid peroxidation
4. Monoxygenases• catecholamine biosynthesis • neuropeptide and neurotransmitter synthesis
5. Dioxygenases• breakdown of L-tyrosine • collagen and elastin synthesis • proteosomal degradation of hypoxia inducible factor-1alpha • salvage pathways • 1st & Last steps in carnitine biosynthesis
6. Histone demethylase• epigenomic regulation • somatic stem cell reprogramming
7. Nucleic acid demethylase• reprogramming of fibroblasts to induced pluripotent stem cells
R. Passwater:You have long been an advocate of the clinical findings of the late fellow North Carolinian, Dr. Fred Klenner, with intravenous vitamin C against several infectious diseases. Why do you find his research so remarkable?

Mike Passwater:Dr. Klenner was a caring physician and a keen physiologist and chemist. He used all the tools available to him in his time to help people throughout his region. He used many treatments including the early sulfa and penicillin antibiotics, as well as oral, intramuscular, and intravenous vitamin C. He developed a preference for vitamin C because it worked well in a variety of situations – toxins, and infections of all varieties. He recognized that vitamin C had diuretic properties and crossed the blood-brain barrier making it an attractive agent in the treatment of brain injuries and infections. He learned that he could safely increase the dosage and frequency as needed to help counteract the presenting challenge. He shared his treatments and results orally and in writing in medical meetings and journals throughout his career. Those who follow his treatment advice have achieved similar results.
It is noteworthy that from the work in the 1930s by Drs. Szent-Györgyi, Svirbely, King, and Waugh to discover and characterize vitamin C, through the work in the current decade by Fowler, Marik, Harrison, Hunninghake, and many others, there has not been a quiet period of vitamin C research or clinical practice. Keep in mind, 48 years passed between James Lind’s discovery that scurvy could be cured with oranges and limes, and lemon juice becoming standard issue on British Navy voyages. Many smart captains traveled with citrus fruit before they were required to do so. It took hundreds of years for hand-washing to catch on as a sepsis prevention tool.
Readers of this column are likely less familiar with the brilliant work of Dr. Richard E. Lee in the Department of Medicine at New York Hospital – Cornell University Medical Center in New York City. In April 1961, the Annals of the New York Academy of Sciences published a summary of his research titled “Ascorbic Acid and the Peripheral Vascular System”(13). The manuscript begins, “Biochemical progress on the investigation of vitamin C has moved with speed since the isolation and identification of this vitamin by King and Waugh.’ Knowledge concerning the basic physiology of its vascular manifestations, however, has failed to keep pace with the progress of chemical information. Even today [1961] we hear the phrases “capillary fragility,” “decreased resistance to trauma,” and “increased capillary permeability,” used in the same relation to the role of vitamin C as they were used nearly 100 years ago, and with little if any more knowledge of meaning or mechanism.” And concludes, “This substance [vitamin C] has been found necessary to maintain responsiveness to stimulation with epinephrine, to maintain the animal’s total vasocompensatory responsiveness and resistance to vascular stress, such as that produced by hemorrhage, and to maintain intact the tonic state of the venules. … The functional pathology scurvy is relieved completely by ascorbic acid feedings but by neither of the two flavonoids mentioned. It is clear from these studies that the peripheral vascular role of ascorbic acid is primarily that of a “tonic,” its absence featured by disturbed function of a widespread symptomatology of great magnitude.”
R. Passwater:Why would vitamin C be effective against sepsis?
Mike Passwater:Vitamin C is necessary for proper functioning of the immune system, along with the vitamin-hormone D, and many other factors. Irwin Stone wrote that fighting an infection without vitamin C is like sending an army into battle without ammunition. Vitamin C and the immune system is a topic unto itself. In advanced sepsis, stabilizing and reversing shock from inflamed, leaky blood vessels is necessary to keep a person alive until the causative situation can be thoroughly treated and resolved.
 In 2017, Dr. John D. Catravas and colleagues shed light on the physiology behind the observations of many others including Drs. Klenner, Lee, McCormick, Fowler, and Marik. (14) In vitro (cell cultures), neither vitamin C alone, nor hydrocortisone (cortisol) alone protected or reversed damage from endothelial barrier insults. However, when the endothelium was treated with both vitamin C and cortisol either before or after insult, endothelial barrier integrity was maintained or restored within minutes.
In 2017, Dr. John D. Catravas and colleagues shed light on the physiology behind the observations of many others including Drs. Klenner, Lee, McCormick, Fowler, and Marik. (14) In vitro (cell cultures), neither vitamin C alone, nor hydrocortisone (cortisol) alone protected or reversed damage from endothelial barrier insults. However, when the endothelium was treated with both vitamin C and cortisol either before or after insult, endothelial barrier integrity was maintained or restored within minutes.R. Passwater:Would it be a good idea for persons with an infection to take vitamin C supplements to lessen the risk of sepsis?
Mike Passwater:The source of infection needs to be removed. Some people will need more assistance than others with this depending on the nature of the infection and the immune status of the person; surgical intervention may be required depending on the situation. The person needs to stay alive to get to and through the treatment. Loading with vitamin C before and during illness is a helpful approach. Including vitamin C as a part of any sepsis intervention protocol is helpful to optimize support of the immune system and the vascular endothelium.
If neutrophils (a type of white blood cell) lack vitamin C, they self-destruct. Instead of fighting the infection or clearing and rebuilding injured tissue, its internal peroxides and enzymes are released damaging the surrounding tissue – like a firefighter using a flame thrower on a housefire.
R. Passwater:What is the latest research with vitamin C against sepsis?
Mike Passwater:Dr. Lee’s work showing the importance of vitamin C to healthy vascular function 60+ years ago was followed decades later by Drs. Armour and Wu, and then Dr. AA Fowler at VCU-MCV published a case series involving intravenous vitamin C in the treatment of acute lung injury in critically ill patients. Dr. Fowler also completed a Phase I clinical trial of the safety of “high dose” IVC in septic patients. The high dose used was 200 mg/kg/24 hrs given for four days (16 grams IVC per day given as four-gram IVC infusions every six hours for an 80 kg adult). Patients were followed for 28 days after the four days of treatment. No patient had an adverse reaction. As expected, all of the septic patients had low plasma ascorbic acid levels at the start of the study (17.9 +/- 2.4 µM [reference range = 50 – 70 µM]). The plasma ascorbic acid levels rose to 1592 – 5722 µM at the end of the four days of IVC treatment. In the IVC group, C-reactive protein and procalcitonin levels (markers of inflammation) were lower, organ failure scores were lower, and thrombomodulin levels (a marker of endothelial damage) did not rise while they did rise in the control group not given IVC.
Dr. Paul Marik in Norfolk, VA, knew of Fowler’s work and tried a similar dose of IVC along with hydrocortisone (cortisol) and vitamin B1 (thiamine), in addition to standard therapy, for a patient with a poor prognosis of surviving. One success led to another, and he and his colleagues have now used a similar approach for over 700 septic patients with impressive results. A couple of clinical trials are enrolling patients, and more are forming, to evaluate protocols similar to Dr. Marik’s.
Like the British ship captains in the late 1700s who embraced citrus fruits before they were mandated, an estimated 20% of intensivists have already adopted similar approaches to Drs. Fowler and Marik. It is noteworthy that vitamin C infusions or injections are not rare, as vitamin C has been a tool for the mitigation of reperfusion injury following cardiac or neurologic procedures for more than two decades. The recent recognition of endothelial dysfunction as a commonality in many life-threatening conditions previously considered unrelated offers exciting possibilities for explaining past successes of early pioneers and offers hope for more successful treatment plans in the future.
R. Passwater:Interesting. This makes a great background review for the clinical studies of Dr. Marik. Let’s chat with Dr. Marik about his clinical success in the next column. Mike, thanks for explaining the biochemistry behind the use of vitamin C against sepsis.WF
Dr. Richard Passwater is the author of more than 45 books and 500 articles on nutrition. Dr. Passwater has been WholeFoods Magazine’s science editor and author of this column since 1984. More information is available on his website, www.drpasswater.com.

References:1. Passwater, R.A. “Oral High-Dose Vitamin C for Major Diseases An Interview with Andrew W. Saul, Ph.D.” Whole Foods (January 2018) https://wholefoodsmagazine.com/columns/vitamin-connection/ oral-high-dose-vitamin-c-major-diseases/ 2. Hershey TB, Kahn JM. State sepsis mandates—a new era for regulation of hospital quality. N Engl J Med [Internet]. 2017 May 21 [cited 2017 June 15]; 376:2311-2313. Available from: https://www.nejm.org/doi/full/10.1056/ NEJMp1611928 doi: 10.1056/NEJMp1611928. 3. https://www.cdc.gov/sepsis/datareports/index.html (accessed June 9, 2018) 4.http://www.wfpiccs.org/wpcontent/uploads/2015/09/2015_WSD_FactSheet_long_English.pdf (accessed June 9, 2018) 5. Prescott, HC., Langa, KM. and Isashyna, TJ. Readmission diagnoses after hospitalization for severe Sepsis and other acute medical conditions. JAMA 313(10):1055-7 (2015) 6. Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med [Internet]. 2013 May; 41(5):1167-74. Available from: https://www.ncbi.nlm. nih.gov/pubmed/23442987 doi: 10.1097/CCM.0b013e31827c09f8. 7. Seymour CW, Rea TD, Kahn JM, Walkey AJ, Yealy DM, Angus DC: Severe sepsis in pre-hospital emergency care: analysis of incidence, care, and outcome. Am J Respir Crit Care Med 2012, 186(12):1264-1271. 17. 8. Singer M, Deutschman CS, Seymour CW, et al: The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA 315:801–810, 2016. 9. Borrelli E, Roux-Lombard P, Grau GE, Girardin E, Ricou B, Dayer JM, Suter PM: Plasma concentrations of cytokines, their soluble receptors, and antioxidant vitamins can predict the development of multiple organ failure in patients at risk. Crit Care Med 1996, 24(3):392–397. PMID: 8625625 Accession: 00003246-199603000-00006. 10. http://www.glycocalyx.nl/background.php (accessed June 19, 2018) 11. Montel-Hagen A, Kinet S, Manel N, Mongellaz C, Prohaska R, Battini JL, Delavnay J, Sitbon M, Taylor N. “Erythrocyte Glut1 Triggers Dehydroascorbic Acid Uptake in Mammals Unable to Synthesize Vitamin C.” Cell 132, 1039-1048, March 21, 2008. 12. May JM, Harrison FE. “Role of Vitamin C in the Function of the Vascular Endothelium”. Antioxidants & Redox Signaling. Vol 19, No 17, 2013. 2068-2083. 13. Lee RE. “Ascorbic Acid and the Peripheral Vascular System” Annals of the New York Academy of Sciences, April 1961. https://doi.org/10.1111/j.1749-6632.1961.tb46129.x. 14. Marik PE, Khangoora V, Rivera R, Hooper MH, Catravas J. “Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study.” Chest 2017 Jun;151(6):1229-1238.
See a comprehensive bibliography atwww.wholefoodsmagazine.com/columns/vitamin-connection.