




Manfred Eggersdorfer, Ph.D. is a professor of healthy aging and holds the chair for healthy aging at the University Medical Center Groningen (UMCG) in the Netherlands and is the senior vice president responsible for nutrition science and advocacy of DSM Nutritional Products, in Kaiseraugst, Switzerland. He studied chemistry at the Technical University Munich and earned his Ph.D. in organic chemistry in the field of synthesis and characterization of unusual amino acids. He completed his post-doc at Stanford University, California, working with Carl Djerassi on the isolation and characterization of sterols from marine origin as potential contraceptives. He joined Roche, Basel, Switzerland in 1999 as head of research and development of vitamins and continued in this capacity after Roche was acquired by DSM in 2003.
Dr. Eggersdorfer’s scientific work focuses on the role of essential nutrients for health, vitality and well-being, especially on the impact of inadequate intake and status of micro-nutrients on long term health and healthy aging. He is active as an advisory board member at the Johns Hopkins Bloomberg School of Public Health, member of the Nutrition Council of Tufts University Friedman School of Nutrition Science & Policy, board member of the Gesellschaft für Angewandte Vitaminforschung e.V. and affiliate of various other organizations. He is the author of numerous publications in the fields of vitamins, innovation in nutritional ingredients and a scientific reviewer for a variety of journals.
Passwater:Professor Eggersdorfer, previously we discussed some of the many actions of vitamin C in the body. How much is the current “officially” recommended dose now? How was this determined?
Eggersdorfer:Such is the challenge; while the existing Food and Agriculture Organization (FAO) and World Health Organization (WHO) guidelines recommend an intake of 45 mg/day (1), current reference values vary from country to country, and are often further influenced by other variables such as age and gender. For instance, the Recommended Dietary Allowance (RDA) in the U.S. was recently revised to 90 mg/day for men and 75 mg/day for women (2). Higher amounts of vitamin C are also recommended for cigarette smokers, pregnant women, and lactating women in the U.S., who are advised to consume an additional 35 mg, 10 mg and 45 mg vitamin C per day, respectively.
Passwater:As we recently discussed with Dr. Andrew Saul, the RDAs for nutrients have been developed to give guidance for nutritional adequacy. They have been prepared by the Food and Nutrition Board since 1941. The first edition was published in 1943 to provide “standards to serve as a goal for good nutrition.” Because RDAs are intended to reflect the best scientific judgment on nutrient allowances for the maintenance of good health and to serve as the basis for evaluating the adequacy of diets of groups of people, the initial publication has been revised periodically to incorporate new scientific knowledge and interpretations.
The 10th edition of the RDAs (1989) defined them as the levels of intake of essential nutrients that, on the basis of scientific knowledge, are judged by the Food and Nutrition Board to be adequate to meet the known nutrient needs of practically all healthy persons. Individuals with special nutritional needs are not covered by the RDAs.

According to the 10th Edition, in principle, RDAs are based on various kinds of evidence: (1) studies of subjects maintained on diets containing low or deficient levels of a nutrient, followed by correction of the deficit with measured amounts of the nutrient; (2) nutrient balance studies that measure nutrient status in relation to intake; (3) biochemical measurements of tissue saturation or adequacy of molecular function in relation to nutrient intake; (4) nutrient intakes of fully breastfed infants and of apparently healthy people from their food supply; (5) epidemiological observations of nutrient status in populations in relation to intake; and (6) in some cases, extrapolation of data from animal experiments. In practice, there are only limited data on which estimates of nutrient requirements can be based.
RDAs have changed over the years as their purpose has changed, but they do not represent the needs for optimal health. This will be discussed in a later column in this series. The RDA for vitamin C is currently 90 milligrams for healthy adults, which is double the original RDA. Please see Table 1.
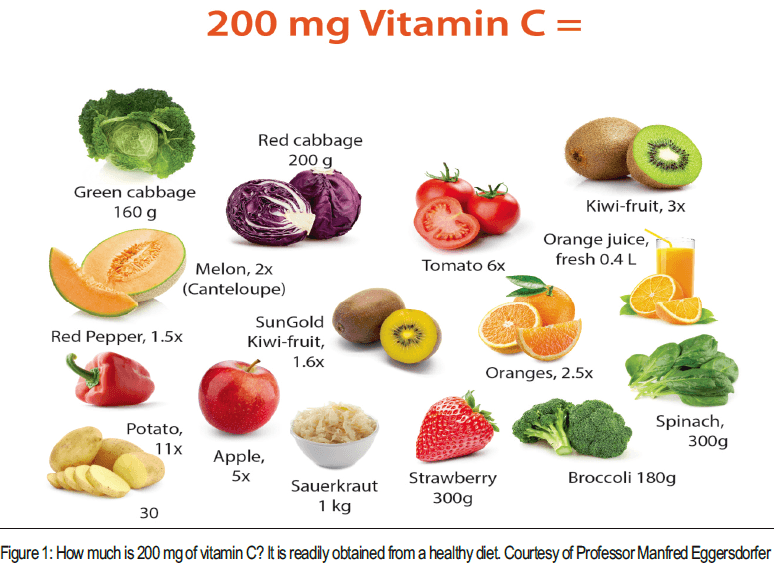
Eggersdorfer:New science is indicating that these recommendations are too low and people miss health benefits that would be achieved by an optimal level. This is the reason countries like China, New Zealand and Australia have developed an additional, so-called “proposed intake” or “suggested dietary target.” While the Recommended Dietary Allowance is set to avoid scurvy as vitamin C deficiency disease, the “proposed intake” is set at 200 mg/day per person to reduce risk for non-communicable diseases (NCDs) like CVD, cancer, and others. With no clear consensus among countries, and the latest scientific recommendations increasingly highlighting the benefits of increased vitamin C intake, it is vital that governments and scientific communities across the globe work together to harmonize vitamin C reference values, thus better supporting global health and immunity.
Passwater:Do data support a higher RDA?
Eggersdorfer:Indeed, the current historic recommendations are based on the level required for scurvy prevention, whereas from the scientific perspective there are well-established arguments for a higher daily vitamin C intake, with 200 mg/day increasingly highlighted as a better reference value. This is based on emerging evidence on the motility of neutrophil leukocytes in relation to vitamin C consumption; neutrophils are essential for the body’s defense against pathogens, and are thought to function best when sufficient vitamin C is available (6,7). As such, they have been identified as an appropriate functional biomarker for benchmarking. Two studies, an in vitro trial, and a human intervention study, have demonstrated an increase in neutrophil motility at a dose of 200 mg of vitamin C and, subsequently, enhanced immunity (8,9). The antioxidant properties of vitamin C mean that higher consumption has also been linked to a reduction in the risk of long-term health
 conditions and non-communicable diseases, such as cardiovascular disease (CVD), particularly when compared with those whose intakes were below the recommended levels (10,11). Based on the evidence from human metabolic, pharmacokinetic, and observational studies and RCTs, 200 mg per day is the optimum dietary intake of vitamin C to maximize the potential health benefits with the least risk of inadequacy or adverse health effects.
conditions and non-communicable diseases, such as cardiovascular disease (CVD), particularly when compared with those whose intakes were below the recommended levels (10,11). Based on the evidence from human metabolic, pharmacokinetic, and observational studies and RCTs, 200 mg per day is the optimum dietary intake of vitamin C to maximize the potential health benefits with the least risk of inadequacy or adverse health effects.Passwater:RCTs are “Randomized controlled trials.” They are studies in which people are allocated at random (by chance alone) to receive one of several clinical interventions. One of these interventions is the standard of comparison or control. The control may be a standard practice, a placebo (“sugar pill”), or no intervention at all.
Eggersdorfer:An intake of 200 mg vitamin C can also be achieved via a balanced diet following the recommendation from WHO and other authorities eating 5-7 servings of fruits and vegetables a day. While the recommended dose of 200 mg can easily be reached via a healthy diet (please see Figure 1), incorporating the five servings of fruit and vegetables recommended by the FAO and WHO per day, changes in modern lifestyles and eating habits, mean that deficiencies are still highly prominent across the globe. This is, in part, due to a lack of discipline in the diet, but is also the result of a widespread association between vitamin C and oranges, when in fact there are a wide variety of other dietary sources. Fortified foods and beverages can also play an important role in helping to address shortfalls of this key vitamin in the diet.
Passwater:Does the efficiency of absorption decrease as the amount ingested increases?
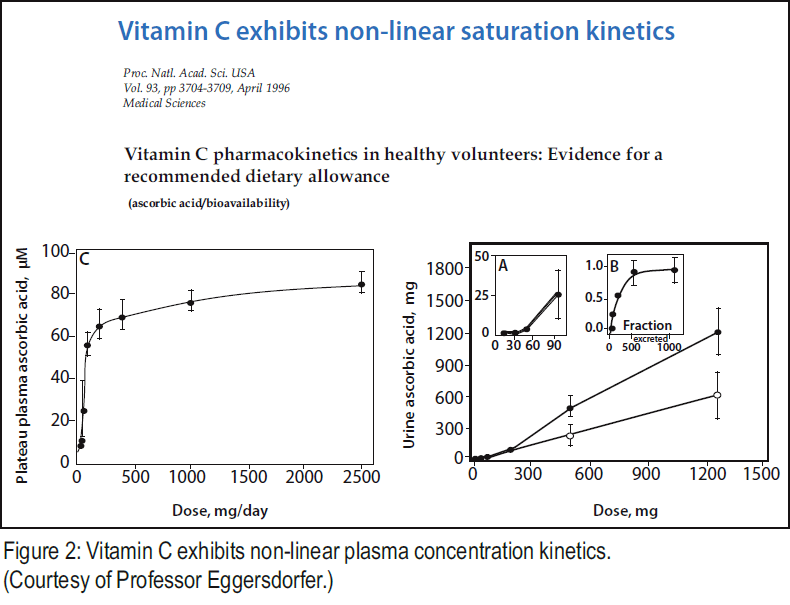
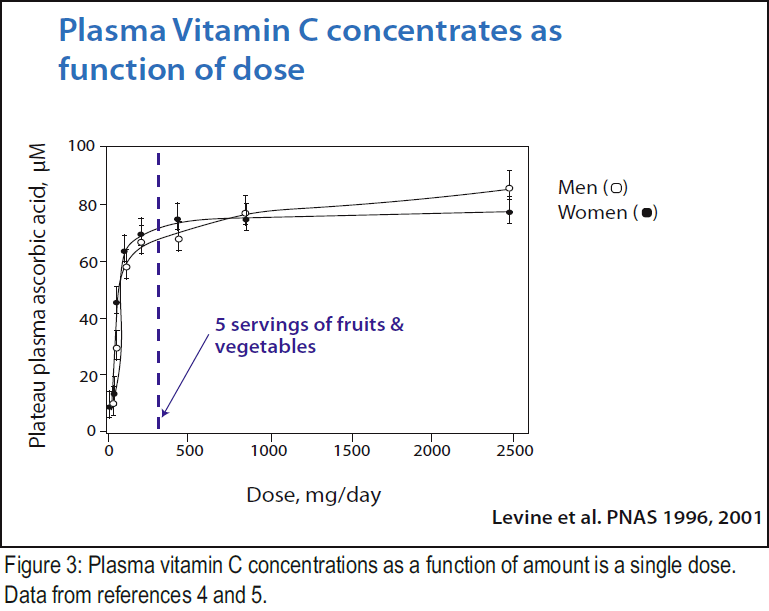
Eggersdorfer:The increasing body of evidence highlights the potential benefits of vitamin C intake in doses exceeding those outlined in current recommendations. At higher intakes, other studies such as those conducted by Dr. Mark Levine et al. of the National Institutes of Health (4), suggest that blood levels plateau. This happens when ingested as a single dose in levels more than 1,000 mg/day. Indeed, plasma vitamin C concentrations appear to be a function of dose, typically displaying sigmoid kinetics. Plasma concentration increases rapidly in doses up to 100 mg/day, and reach a near steady-state level for a single dose above 1,000 mg. In summary, vitamins start to decrease at higher dosage (4,5) Please see Figures 2 and 3.
Passwater:These data reflect single dose efficiency only. When the total amount is divided into several doses, then even more — a greater percentage and greater total amount — of vitamin C is absorbed (12). Also, these studies reflect only the results from a very small number of subjects. We will discuss the differences in absorption between single-dose and multiple dosages spread over time in next month’s column.
Why does the efficiency of absorption decrease?
Eggersdorfer:There is a tight control of vitamin C plasma level. Vitamin C is absorbed by specific transporters, which manage the uptake from the intestine. So even with higher intakes, the vitamin C does not reach the plasma as the uptake and transport is limited by the transporter capacity. Interestingly, the kidneys also play an important role in regulating plasma vitamin C concentration; when intake is insufficient, the body triggers renal re- absorption to avoid too low of a plasma level.
Passwater:Does a diminished rate of absorption mean the cells are saturated with vitamin C?
Eggersdorfer:A diminished rate of absorption only occurs at higher doses, and to the current knowledge is independent from cell or tissue saturation. The rate of absorption and bioavailability depends only on the dose of vitamin C, due to the limited capacity of the specific vitamin C transporters (SVCT1) in the small intestine. This is the reason — for certain applications — intravenous doses are used. Oral doses of up to 200 mg are absorbed almost completely, and at higher doses, absorption declines so that less than 50% is absorbed at a dose of 1250 mg (4).
Passwater:That’s still more vitamin C absorbed (625 mg vs. 200 mg). This can be an important increase. Dividing the vitamin C into several doses throughout the day can result in even more vitamin C being absorbed from the same amount taken.
Could there be health benefits from intakes higher than 200 mg?
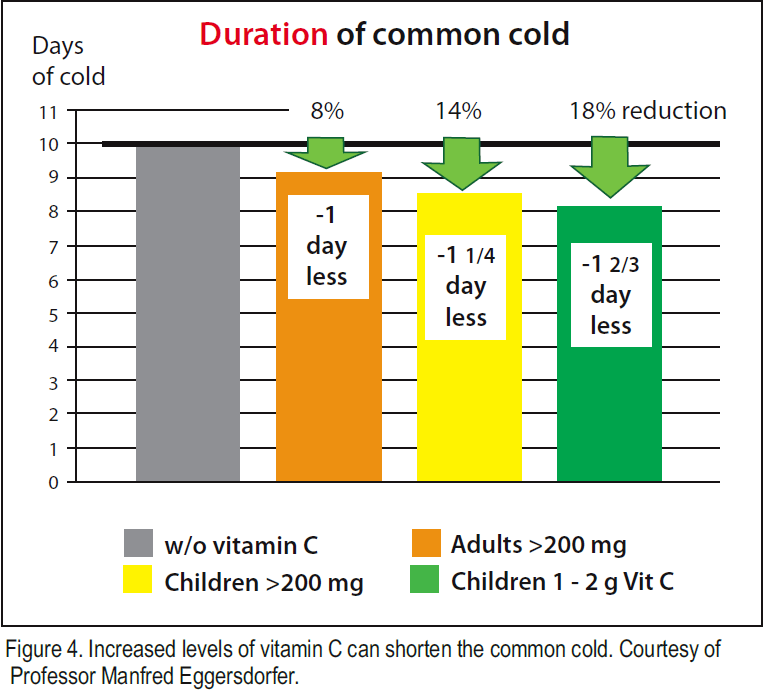
Eggersdorfer:Yes, indeed, there are studies showing that vitamin C intake in dosages higher than 200 mg may have further beneficial effects. For example, in the January 2013 Cochrane review by Hemilä (13) on the link between vitamin C supplementation and the common cold, a reduction in the duration of common cold symptoms was observed in children when ingested in doses of 1-2 g/day. Even if only part of a higher dose is required and absorbed by the body, it will help to increase plasma concentration levels and ensure tissue saturation. This benefit of vitamin C is important as there are no remedies to fight common cold. Higher doses above the UL (Tolerable Upper intake level) which is set at 2,000 mg by the Institute of Medicine (IoM) are not recommended for nutritional purposes, due to a potential increased risk of intestinal discomfort and disturbances like diarrhea. However, doses above 2,000 mg may be a choice in certain applications under medical supervision.
Passwater:I want to remind our readers that the UL is NOT the limit for safe intake, but is merely the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects to almost all individuals in the general population. I have been taking 4,000 mg of vitamin C daily since the 1960s with no adverse effects. Whenever I am subjected to people having colds or flu, I change to a gram (1,000 mg) each hour during my waking hours and have had no adverse effects.
The 2000 RDA for vitamin C set a tolerable upper intake level (UL) for vitamin C for the first time. A UL of 2 grams (2,000 milligrams) daily was recommended in order to prevent most adults from experiencing diarrhea and gastrointestinal disturbances. The 2000 RDA

publication for vitamin C states: “The Tolerable Upper Intake Level (UL) is the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects in almost all individuals. Although members of the general population should be advised not to exceed the UL routinely, intake above the UL may be appropriate for investigation within well-controlled clinical trials. In light of evaluating possible benefits to health, clinical trials of doses above the UL should not be discouraged, as long as subjects participating in these trials have signed informed consent documents regarding possible toxicity and as long as these trials employ appropriate safety monitoring of trial subjects. Also, the UL is not meant to apply to individuals who are receiving vitamin C under medical supervision” (14).
Professor Eggersdorfer, thanks for discussing the RDA for Vitamin C. Next month, let’s discuss the safety and benefits of really high levels of vitamin C in the blood that can only be achieved by IV vitamin C. WF
References
1) Food and Agriculture Organization; World Health Organization,Human Vitamin and Mineral Requirements; Training Materials for Agricultural Planning, Bangkok, Thailand, 2002.
- Institute of Medicine. “Dietary Reference Intakes of Vitamin C, Vitamin E, Selenium, and Carotenoids;” Washington, DC, USA, National Academic Press, 2000
- Levin et al. JAMA 2006.
- M. Levine et al., ‘A new recommended dietary allowance of vitamin C for healthy young women’, Proceedings of the National Academy of Science of the United States of America, vol. 98, no. 17, 2001, p. 9842-9846,
- M. Levine et al., ‘Vitamin C pharmacokinetics in healthy volunteers: evidence for a recommended dietary allowance’, Proceedings of the National Academy of Science of the United States of America, vol. 93, no. 8, 1996, p. 3704-3709.
- L. A. Boxer et al., ‘Enhancement of chemotactic response and microtubule assembly in human leukocytes by ascorbic acid,’ Journal of Cellular Physiology, vol. 100, no. 1, 1979, p.119-126
- V. Elste et al., ‘Emerging evidence on neutrophil motility supporting its usefulness to define vitamin C intake requirements,’ Nutrients, vol. 9, no. 503, 2017, p.1-16
- J. Schwager et al., ‘Ascorbic acid modulates cell migration in differentiated HL-60 cells and peripheral blood leukocytes’. Molecular Nutrition & Food Research, vol. 59, no. 8, 2015, p.1513-1523
- S. M. Bozonet et al., ‘Enhanced human neutrophil vitamin C status, chemotaxis and oxidant generation following dietary supplementation with vitamin C-rich sungold kiwifruit,’ Nutrients, vol. 7, no. 4, 2015, p.2574-2588.
- Enstrom et al., ‘Vitamin C intake and mortality among a sample of the United States population,’ Epidemiology, vol. 3, no. 3, 1992, p.194-202
- N. R. Sahyoun et al., ‘Carotenoids, vitamins C and E, and mortality in an elderly population, American Journal of Epidemiology, vol. 144, no. 5, 1996, p.501-511
- Hickey, S. & Roberts, H. “Ascorbate: The Science of Vitamin C.” Lulu publ. ISBN 1-4116-0724-4 (2004).
- Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev. 2013 Jan 31;(1):CD000980. doi: 10.1002/14651858.CD000980.pub4.
- Food and Nutrition Board, Institute of Medicine. “Vitamin C. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids. “Washington, D.C.: National Academy Press; 2000:95-185.

Published in WholeFoods Magazine February 2018







